Issue:March 2016
PULMONARY DELIVERY - Afrezza – Another Lesson for Drug Delivery Professionals?
INTRODUCTION
Often when discussing financial and geopolitical events, we use the expressions “history repeats itself” and “those who do not learn from history are fated to repeat it.” But perhaps a more realistic assessment is offered by the statement that “history doesn’t repeat itself, but it does rhyme.” Mannkind’s recent announcement that Sanofi has decided to return the marketing rights for Afrezza may not exactly be history repeating itself, but it certainly feels as though it rhymes.
The challenges in successfully introducing an inhaled insulin product shouldn’t be a surprise to anyone who follows the pharmaceutical industry. The first inhaled insulin product, Nektar and Pfizer’s Exubera, was launched a decade ago with much fanfare and investment but little success. A year later, 2007, Exubera was withdrawn from the market. The general sentiment regarding its failure was that the dry powder delivery device, a large bong-shaped apparatus, was too large and unwieldy. This, combined with respiratory function testing requirements, seemed the obvious reasons for a multibillion dollar product failure. There were no quick fixes; a device redesign would take a couple of years along with several million dollars to reengineer, manufacture, and clinically validate. Easing the requirement for respiratory function testing would take even longer and require years of positive patient experience. Neither of these challenges were easy, inexpensive, or short-term. In the end, Nektar and Pfizer decided to withdraw the product, and Nektar wrapped up its inhaled insulin program, shut down its inhalation activities, and sold the assets to Novartis.
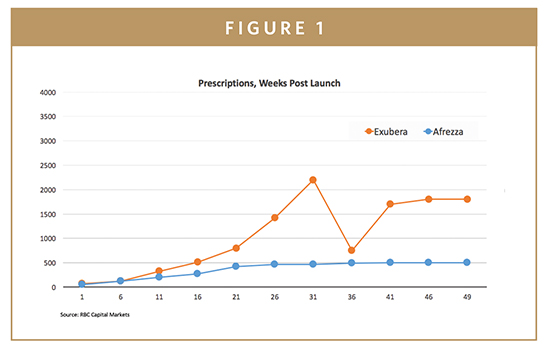
During this 2006-2007 period, Mannkind had entered Phase III testing with their dry powder insulin and were faced with a critical decision. Mannkind had by then invested almost $750 million in R&D, largely to develop their inhaled insulin, a figure that has since ballooned to about $1.8 billion. In retrospect, it seems Mannkind was confident that their product would be able to succeed largely by overcoming the most obvious shortcoming of Exubera, an unwieldy device. Unfortunately, following US approval in 2014 and first sales in 2015, the market hasn’t agreed with their optimism and uptake of Afrezza, as measured by sales and prescriptions, has lagged considerably behind the corresponding performance of Exubera a decade earlier.
Mannkind has declared their intention to soldier on with Afrezza, perhaps finding a new marketing partner. They really don’t have much choice if they want to succeed with Afrezza. Like Nektar and Pfizer a decade earlier, there is no quick, easy, cheap fix. Perhaps success can be found by allowing physicians and patients sufficient time to experience the benefits of Afrezza. The product may still earn enough to keep the company alive, if not pay off its development costs.
What are the lessons to be learned from the experiences of Mannkind and Nektar in the area of inhaled insulin? If we pay close attention, it seems we can sense familiar rhymes and rhythms, which if understood can provide guidance for future products targeted to treating systemic diseases using the lung Drug Delivery organizations, in partnership with first-class Big Pharma partners, have failed to crack the inhaled insulin opportunity. And Mannkind a decade later had the benefit of understanding the Exubera experience. Inhaled insulin is seemingly a tough challenge from a formulation, clinical, and commercialization perspective.
Afrezza seemed to have checked off all the boxes in terms of optimizing the pulmonary delivery of insulin, but still missed the mark. Will inhalation ever be a reasonable delivery option for the systemic delivery of insulin? What about any other inhaled pharmaceutical targeting a systemic indication? Is the lung even a reasonable systemic delivery portal for small molecules in an acute setting? While acute indications would seem to be the most obvious opportunity, there are no product successes to look to, even with small molecules. With the exception of Alexza’s struggling Adusave for agitation, inhalation products are being used solely for locoregional pulmonary indications that range from asthma, COPD, and infectious disease to cystic fibrosis, localized cancers, and pulmonary arterial hypertension. A number of inhalation products that were intended to treat systemic conditions, such as acute pain, migraine, and erectile dysfunction, have faded away in the clinical setting.
Looking a little more closely, one can discern certain elements in the Afrezza story that seem to rhyme with previous experience and may offer some suggestions for future product development targeted to pulmonary delivery.
THE BOTTOM LINE IS SAFETY
The Hippocratic oath includes the declaration “I will utterly reject harm and mischief.” That encapsulates one of the key considerations in any physician’s decision. Does a new medication enhance safety, or at least not compromise safety? Is any improvement in efficacy or convenience offset by a loss in safety or tolerability? In the case of doubt, the default position for most physicians seems to be avoid the new and continue with products they know and trust. And most physicians, the classical Early and Late Adopters, are exactly the target group that any product needs to capture if it is to be successful. In the case of Afrezza, the lung is not the target organ, but it might be the one to suffer. Patients can’t live without their lungs.
BALANCE RISKS WITH BENEFITS WHEN IDENTIFYING OPPORTUNITIES
Improved convenience is great if there is no compromise in efficacy or safety. Greater convenience might even improve efficacy if it improves compliance. Novel delivery approaches, especially those with any type of inherent risk, are perhaps better off initially targeting high-need indications, in which there may be a more relaxed risk/benefit threshold.
THE LUNG IS DIFFERENT
The lung is not like the skin, the nose, or even the stomach. Delivery to the skin offers a number of safety benefits. It presents a large surface area that permits delivery sites to be rotated, and it is also easily inspected for tolerability and safety issues by the health professional and the patient. In a worst-case situation, sections of skin can be removed and repaired with grafts. Delivery to the lung is a bit of a black hole. Selective delivery to distinct areas of the lung is hard to accomplish, rotating pulmonary delivery sites is hard to imagine, and assessing ongoing safety can only be performed through indirect testing. There is no simple “look- and-see” approach to head off more serious problems.
START WITH ACUTE & MOVE TO CHRONIC
When developing applications for a novel delivery system, it’s tempting to jump right in and address a chronic medical condition. Chronic treatment can lead to long-term use and commercial success. It also leads to more scrutiny and concern about long-term toxicity. Inhaled insulin has been shown to cause a slight decrease in lung function over the short-term that doesn’t seem to get worse, or better, over a 2-year period. Will additional years of use further compromise lung function? Might chronic inhaled lead to other risks? Possibly not, but many issues need to be carefully considered when starting with any chronic therapy. Starting with an acute indication can often reveal and validate the usefulness of a delivery system, while building a safety database that helps support eventual chronic use.
INJECTION IS AN INCREASINGLY ATTRACTIVE OPTION
Gone are the wide bore needles and the pain, the ampoules, vials, and the need to fill a syringe. Today’s options make self-injection, at least subcutaneous injection, reasonably convenient and comfortable. And with the ability to rotate injection sites, there is little concern about local tolerability. Combined with reliable systemic delivery performance, and limited concerns about significant local tissue toxicity, injection has become a very acceptable delivery route for patients once they get over the “ick” factor of self-injection.
TIME & COMPETITION DO NOT STAND STILL
Afrezza has been in development in one form or another for the better part of 2 decades. The product was in late Phase II trials in 2004, a year before the launch of Exubera. Will a compelling product opportunity in 2004 still be compelling a decade later? The challenge for any Project Team starting from scratch is not to imagine the best product today, but the best product at the time of launch. That may be as much as 10 or 15 years later. New Product Teams need to become futurists and realists with respect to development times if they have hopes of their product succeeding in the marketplace.
FIND A WAVE & RIDE IT
If necessary, create a wave to ride. Successful products are generally launched with momentum, what might be considered a wave of excitement and latent support. Riding a tall wave can generate product awareness, trial, experience, and rapid adoption. Exubera rode a wave of expectation that it would free patients from the need for daily injections. Unfortunately, that wave was either not big enough or crashed on the rocks of safety and price concerns before it could be fully exploited. This may explain why Afrezza, arguably an improvement on Exubera, has not been able to reach even the level of prescriptions and sales achieved by Exubera. There is no longer any wave of excitement and anticipation for an inhaled insulin.
Delivery to the lung is a challenge for Drug Delivery Professionals from both a device and formulation perspective, even when addressing locoregional applications. The challenges are much greater when using the lung as a portal for systemic delivery. Future success in delivering insulin via the lung, or any other pharmaceutical, will depend on managing the many technical, clinical, and regulatory challenges, while meeting physician and patient expectations. Understanding history and what has come before can provide important insights to help align reality with expectations. But even great design and execution can fall short for no apparent rhyme or reason.
To view this issue and all back issues online, please visit www.drug-dev.com.
Dr. Josef Bossart is Managing Director of Pharmanumbers, a Drug Delivery and Formulation specialty group that helps clients understand, and communicate, how products and technologies can be best positioned for commercial success. He also serves as Executive Editor with PharmaCircle LLC, a trusted resource and full-service solution delivering authoritative content, global insight, and expert analysis on the pharmaceutical, biotechnology, medical device, and animal health industries. Dr. Bossart has more than 3 decades of pharmaceutical industry experience in a variety of roles ranging from sales to marketing to business development to general management. He earned his PhD from the College of Pharmacy, The Ohio State University.
Total Page Views: 1860