Issue:January/February 2017
COMBINATION PRODUCTS - 6 Guidelines to Follow When Developing Combination Products
INTRODUCTION
While the development of a combination product comes with significant patient benefits through technology and molecule innovation, that reward can be offset by the range of regulatory complexity and uncertainty encountered with bringing a product to market, in addition to any post-marketing activities. The area of combination products is still unique to many regulatory authorities abroad, wherein the lines are often blurred when it comes to product classification and jurisdiction. While the regulatory path and compliance requirements may be fairly clear in one country, there are no universal templates, procedures, or exacting opinions to follow for harmonized solutions.
Combination products have the potential for significant therapeutic advantages over traditional dosage forms of medicine by delivering value and convenience for both patient and point-of-care provider, maintaining dosage compliance, and providing novel drug delivery therapies for unmet medical needs. Combination products, such as in vitro diagnostics and radio-biologics, have been on the market since the 1970s. However, there has been a proliferation of combination product platforms that have been developed throughout the years covering a wide range of drug delivery applications. The main drivers for the increasing demand of these novel therapies are customer convenience, evolving medicine models, and reimbursement strategies, and the increasing demand for product intelligence features. Current trends in healthcare toward more outpatient and home-health-based services have only accentuated those needs.
In 2013 alone, there were 313 Combination Product Applications submitted to the FDA. Roughly 88% of these applications were divided, from a reviewing standpoint, fairly evenly between CDRH and CDER.1 But despite the increase in the development of these device platforms, regulatory authorities are still struggling to identify if these products are drugs, devices, or both. Sponsor companies can reduce the risk and impact that regulatory uncertainty can play by, in advance of pursuing development, understanding the regulatory landscape and then developing a regulatory compliance strategy that is appropriate and suitable for the combination product as a “system.” The following six guidelines will help reduce the number of questions coming back from the reviewing agency, thereby enabling speed to market.
DEFINE THE PMOA (ACCURATELY)
Have a clear understanding of all applicable regulations, guidance documents, and any predicate products prior to developing a regulatory and quality compliance strategy. Early and meaningful engagement of the respective regulatory reviewing office is also key to avoiding delays and submission refusals. The primary US FDA-applicable regulations can be found in FDA 21CFR Part 3 and Part 4, along with 13 primary FDA Guidance Documents. A recent FDA performance report concluded that from 2009-2014, there were 67 requests for designation (RFD) for formal combination product classifications and assignments. Of those 67 RFDs, 69% were found to have been insufficient with the information provided by the sponsor. Another 6% of the filings were withdrawn by the sponsor prior to the issuance of a decision.2 One common mistake made by sponsors when filing an RFD is failing to distinguish between the primary mode of action (PMOA – often the most important therapeutic action) and multiple modes of action with reasonable certainty (21 CFR Part 3.2). Depending on the constituent parts of the overall combination product system, there can potentially be multiple modes of action. Clearly defining the PMOA is critical to obtain approval at first pass. If the sponsor cannot define with certainty the PMOA, then the FDA will likely use the PMOA assignment algorithm. The assignment then comes down to historical precedents and the respective FDA office with the most experience for the product in question.
RESEARCH THE GLOBAL REGULATORY GUIDELINES
Though the path for combination product regulatory approval in the US (FDA) is more defined and currently evolving, there is little harmonization with the rest of world. For example, if a sponsor wanted to file for market approval in Europe, there is no specific, centralized decision-making body that will provide a clear understanding of filing requirements. For Europe, MEDDEV 2.1/3 establishes clinical data submission considerations, but still falls short in describing the clear regulatory path the product must progress through in order to obtain a favorable opinion.3 Latin American countries, such as Brazil, have no specific combination product regulations. Sponsor applications for these products would currently fall under Brazilian, Federal Laws No. 5.991/73 and 6.360/76 and ANVISA’s (the Brazilian National Health Surveillance Agency) Decree No. 79.094/77, which regulates both drugs and medical devices. Additionally, Law No 5.991/73 outlines the requirements for what is considered a product intended for medicinal purposes, those that are medical devices, and those that may warrant a pre-review by the Brazilian Ministry of Health and ANVISA.4
The advice here is to get engaged early with any potential country where you plan to do commerce. Gaining clarity on national requirements may not be enough. The sponsoring company may need to drill down to the regional and local jurisdictions to fully understand all requirements and nuances. This level of granularity is especially important if you choose to conduct clinical trials overseas, with clinical trial materials made in another country. In these cases, import/export laws must be considered and planned. This is where having regionally deployed personnel (“boots on the ground”) are effective for navigating the regulatory waters of local jurisdiction.
DEVELOP AN APPROPRIATE CGMP QUALITY COMPLIANCE STRATEGY
From a quality systems standpoint, combination products should be viewed holistically as a “system” in which both constituent parts must have suitable quality system requirements in place, be it manufactured in the same facility, different facilities, or completely outsourced (virtual sourcing). We find through various FDA Form 483(s) (Warning Letters and other recent stark reminders, that the development and understanding of a combination product is sometimes not in synch with the cGMP manufacturing strategy. For example, in 2014, the FDA issued a Warning Letter to Amgen as a result of a June 2014 inspection related to the PROLIA prefilled syringe and needle guard, ENBREL lyophilized vial and diluent with vial adaptor, and Enbrel prefilled syringe with SureClick 1.5 auto injector.5 Deficiencies cited were primarily in the quality system element areas of design controls, change controls, and purchasing controls. The interpretation of this Warning Letter would suggest that systems need to be developed and acted on for both device and pharmaceutical/biologic types. The Warning Letter also infers that legacy combination products that are still on the market may be held to a more rigorous standard in the near future, including the retrospective application of medical device and/or pharmaceutical quality system requirements. The Quality Management System (QMS) should be derived by a blended or bolt-on approach. If the sponsor is a pharmaceutical company that develops combination products and conducts or provides oversight for device operations, then build in those device requirements into the pharma-based model for complete regulatory compliance coverage. Likewise, if the sponsor is a device manufacturer that conducts or provides oversight for pharma operations, include the device requirements. It is often good to coach people on the idea that both worlds are not mutually exclusive. Strip the label off of the (device or drug) regulation and focus on the actual intent of what is being requested in the requirement.
IMPLEMENT A DESIGN FREEZE DURING THE COMBINATION PRODUCT DEVELOPMENT PROCESS
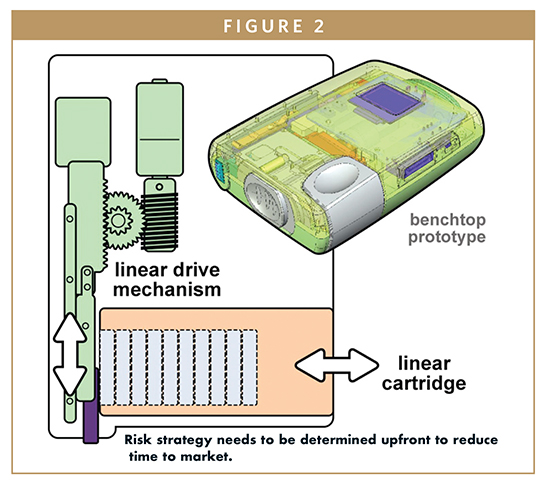
Pharma and biologics companies are not device companies, and thus, many are unfamiliar with the concept of a “design freeze.” The freeze is the point in the product development life cycle at which the actual design has been formally approved and all product changes are prohibited, unless initiated through the design control process. Knowing when to do a design freeze during the development of a combination product is critical. Typically, a design freeze is initiated just before the validation/verification stage of a medical device. Any changes that are made to the device design post design freeze, and once initial data has been submitted for regulatory review, may trigger additional requirements of the design outputs. Ideally, sponsor companies should think about incorporating clinical studies (including human factors) prior to implementing the design freeze. By implementing a development pilot study prior to any pivotal clinical trial, the sponsor company can gain valuable insight into product performance. If the product remains consistent and robust throughout the studies, the data could feasibly be used to propel the product ahead of plan.
Sometimes, pharma companies, in general, are reluctant to change a device once it is on the market because that usually results in additional clinical studies and a significant amount of money and time to resubmit. Regulatory delays can be significant for a combination product worth several million dollars. Conversely, some device companies seem to have an affinity for making changes to a device; they want the next generation, better ergonomics, with more human factor studies.
The design freeze is extremely important because if the design keeps changing and there is no stage-gate or control built into the process, sponsor companies will find it difficult knowing what to incorporate for design reviews, design verification protocols, and subsequent validation data. Regulators want to see a firm plan with traceability from the base level of design (proof-of-concept). They also want to ensure that the device they are approving is just as safe and effective as the constituent drug/biologic part, from a clinical standpoint. Do not be surprised during the submission process if additional clinical data is requested above what was already submitted.
USE RISK-BASED DECISION MAKING TO DEVELOP & BRING THE PRODUCT TO MARKET
Any type of risk, such as the potential harm the device could cause to the patient, has to be considered when developing a combination product. Use failure modes and effect analysis to look at all the risk in the development for both the individual constituent parts and the system as a whole.
For instance, when the drug/biologic target product profile (TPP) is being established, the sponsor company can, in parallel, integrate the device design development concept into this discussion by asking how using a certain material in the manufacturing of the device could possibly introduce a leachable/extractable that would pose significant harm or risk to patient, and stability profile of the product. As an example of this thinking, consider a sponsor company working with a device design and development company to produce an insulin auto-injector. The next-generation auto-injector may require an option for changing the grade or properties of a polymer or a resin additive. Using risk-based decision-making, the two companies would need to work together to determine if they would have to go back and complete biocompatibility studies with the resin change and the drug to see if they were compatible.
It really comes down to determining what risk strategy the sponsor company will employ in the development of the combination product, and will the sponsor company deploy it in separate parts – one for the drug and one for the device. Or, is it going to be a combined strategy in which the drug and device companies are working together in planning the development?
ESTABLISH A PRODUCT STABILITY STRATEGY
The FDA and EU want to see stability studies on file before a final submission is sent to them. Determine if the device and drug should be studied with the two components together, independent of one another, or both. Analyze how or if the device changes the actual drug once the two are paired together over the shelf-life of the product. The sponsor company will need to provide details of these studies and validation that the products are safe for patient consumption before the regulatory bodies will consider approving. You also need to consider what specific tests need to be performed on each constituent part and together as a system. For instance, if the company is performing shock and vibration studies on a particular drug delivery device, should they do this separate from the drug being included, together, or both? If conducting accelerated aging on a system or constituent products, is the company carrying out physical testing and then monitoring all relevant time points? Is stability ending at the end of shelf-life only, or does the company go past expiry? All are factors that should be included in a sound stability strategy.
CONCLUDING ADVICE
The regulatory submission and approval process for combination and drug delivery devices is still evolving, which means sponsor companies may have a lot of unanswered questions. Implementing some of the aforementioned essential guidelines is key to improving the odds of first-time regulatory approval. Many companies file with not enough or the wrong information, or they don’t establish an appropriate QMS, all of which slows their approval process and costs them more time and money. Speed to market is then lost. The more meaningful data the sponsor company has that validates the product as a system, and the more sound and holistic the product development and cGMP processes are, the better the chances are of first-time approval, which ultimately saves the sponsor company both time and money.
REFERENCES
1. Food and Drug Administration: FY 2014 Performance Report to Congress- Office of Combination Products (Required by the Medical Device User Fee and Modernization Act of 2002).
2. Ibid.
3. EUROPEAN COMMISSION: Guidelines on Medical Devices: Clinical Evaluation: A Guide for Manufacturers and Notified Bodies, MEDDEV. 2.7.1 Rev.3 (December 2009).
4. Medical Devices BRAZIL Demarest e Almedia Advogados: Lex Mundi Publication. 2011.
5. Chimera Consulting, North America, LLC. Summary of Key Points: Warning Letter to Amgen 2014 (PROLIA Prefilled Syringe and Needle Guard, ENBREL Lyophilized Vial and Diluent with Vial Adaptor, and Enbrel Prefilled Syringe).
To view this issue and all back issues online, please visit www.drug-dev.com.

Winston Brown is the VP of Global Quality at Phillips-Medisize. He has more than 20 years of experience in global Quality, Regulatory Compliance, and Operations working with diverse pharmaceutical, medical device, biologic companies. He can be reached via email at Winston.Brown@phillipsmedisize.com.
Total Page Views: 3577